

How It Started
Maple's owners first noticed a lump on her right forelimb, just above the elbow, two weeks prior to being admitted to Advanced London Vetcare. A fine needle aspirate confirmed a mast cell tumour, and she underwent surgical removal at her local veterinary practice. The mass had appeared relatively superficial, but during the course of her surgery it proved deeper than expected.
In the days after surgery, things didn't go to plan. Swelling appeared almost immediately after her bandage was removed and over the following weekend a small wound gap grew into something much more concerning. By the time Maple was referred to Advanced Vetcare London on 4th February 2026, her wound had broken down almost entirely - a process known as wound dehiscence.

What We Found
On examination, the wound extended from the front of Maple's upper arm all the way down to the antecubital fossa (the area in front of the elbow). The edges were necrotic, remnants of the original sutures were still in place and there was heavy purulent discharge tracking down the lower limb.
"Most likely there was just too much tension on the wound and it broke down and got infected," explains Mr. Jakub Köcher-Vodnárek, soft tissue surgery specialist at Advanced Vetcare London who led Maple’s treatment.
"The referring practice had already taken swabs, so we knew which bacteria we were dealing with - staphylococci and streptococci, both sensitive to the antibiotics already in use."
Samples taken from multiple areas of the wound bed in-house showed no evidence of residual mast cells which was reassuring news, given that histopathological examination had already confirmed complete excision of the original tumour.
Phase One: Stabilising Maple’s Wound
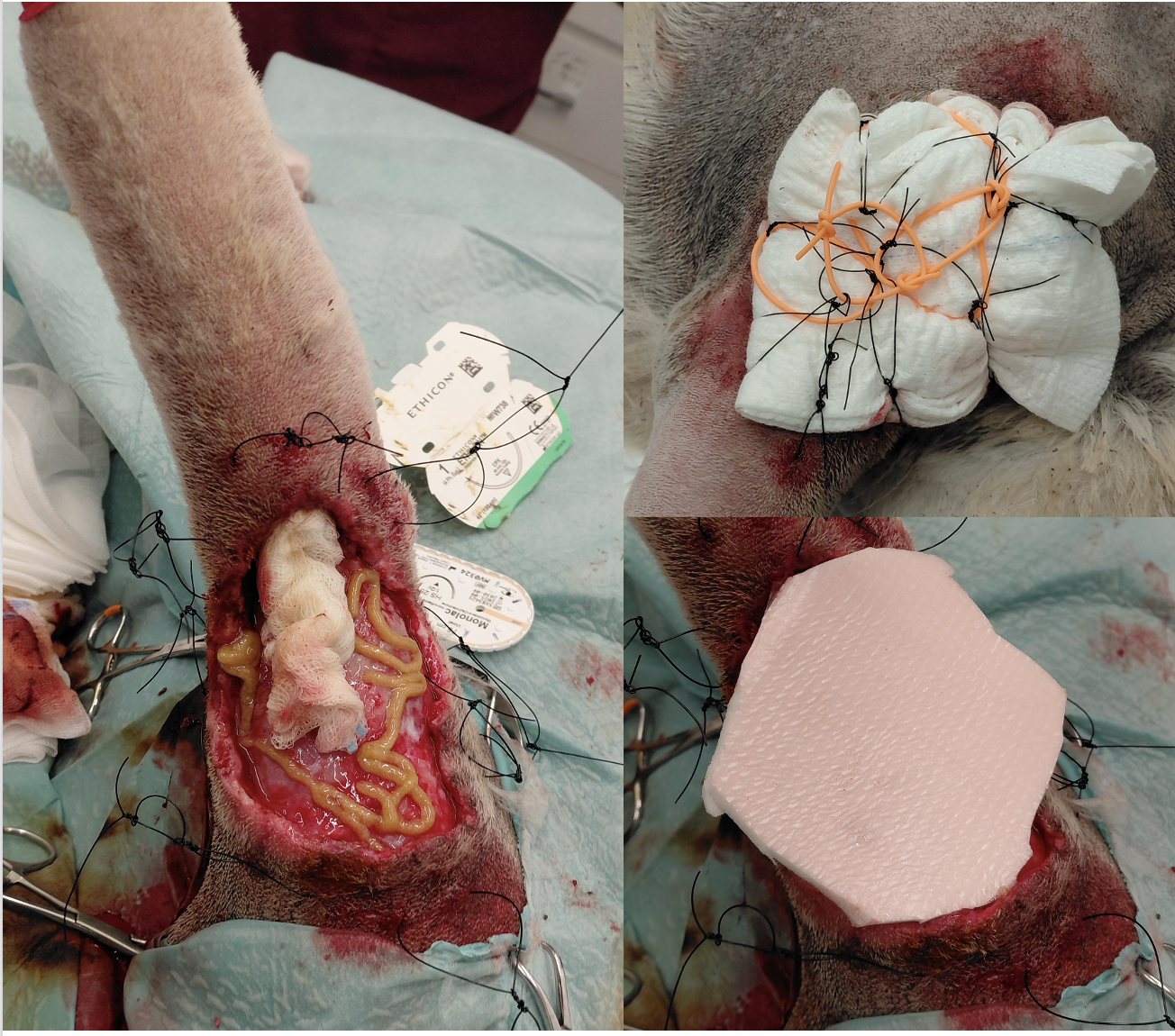
Before any surgical repair could be considered, the wound environment needed to be brought under control. Our team began with careful debridement of all necrotic tissue, copious lavage, and identification of a fluid-filled pocket tracking down towards the lower limb, which was packed with iodine-soaked gauze.
To protect the cleaned wound bed and keep it moist, a tie-over bandage was applied - a technique that uses sutures placed around the wound margins to secure a dressing firmly in place over wounds located in areas where adhesion is difficult, such as the upper limb.
Maple was hospitalised, and the bandage was changed every six hours. Over two days, the wound environment began to improve. Healthy pink granulation tissue began to develop, suggesting the early signs of healing.

Phase Two: Negative Pressure Wound Therapy
With early improvement visible, the team made the decision to transition to negative pressure wound therapy (NPWT), sometimes referred to as VAC (Vacuum-Assisted Closure) therapy.
"NPWT uses gentle, constant suction on the wound," says Jakub. "It helps to heal wounds faster by removing excess fluid, reducing infection risk and improving blood flow which brings the healing cells directly to the wound. It also keeps the wound clean and protected, and because the dressing can stay in place for several days at a time, it's less disruptive for the patient."
A KCI black foam dressing was sutured in place and negative pressure set to 100 mmHg once a seal was achieved. Remarkably, Maple was discharged home the same day with the VAC machine accompanying her allowing her to recover in a familiar environment.
Her owners were given clear instructions: the machine must not be switched off for longer than two hours, and they managed one minor sealing incident confidently at home. By the time Maple returned four days later, two full canisters had filled with discharge - a clear sign of how much the therapy had drawn from the wound.

Phase Three: Surgical Reconstruction
Maple returned on 10th February for VAC removal and definitive surgical closure. When the dressing came off, the transformation was striking: healthy granulation tissue had filled almost the entire wound bed, with only a small area of fatty necrosis remaining at the edge of the lower limb.
The wound edges and bed were refreshed, the necrotic tissue removed, and the area thoroughly cleaned. The team then prepared for the reconstructive element of the procedure.
"Because of where the wound was, over the front of Maple’s elbow, direct closure simply wasn't possible without creating enormous tension," explains Jakub. "We used a technique called a thoracodorsal axial pattern flap, whereby a nearby "patch" of skin, still connected to its own blood supply through the thoracodorsal artery and vein, was gently lifted and rotated 180 degrees to cover the wound on Maple’s elbow.”
The flap was secured with interrupted sutures, a drain was placed to manage any residual fluid, and the donor site was closed. Maple recovered smoothly from anaesthesia and went home the same evening.

The Recovery
Flap surgery requires a careful post-operative period. Maple's owners were asked to apply gentle cooling pads over the flap three times daily in the first 24 hours — a precaution to support circulation in the early stages of flap integration. Strict rest, short toileting walks only, and a protective collar to prevent licking were all part of the plan.
As is common with flap reconstruction, some discolouration and swelling of the flap was expected in the first few days, and a small revision was needed to address a section of the flap tip that did not fully survive - a well-recognised and manageable complication of this type of surgery.
"The distal tip of the flap not surviving is very common," notes Jakub. "We were able to address that in a small second procedure. And from there, the healing was straightforward."
The final suture removal marked the end of Maple's treatment journey and the beginning of her return to normal life.

What This Case Teaches Us
Maple's case is a good example of why staged wound management matters. Attempting to close an infected, necrotic wound primarily, however tempting, risks failure. By taking the time to first clean and stabilise, then use NPWT to optimise the wound bed, and finally reconstruct once conditions were ideal, the team gave the repair the best possible foundation.
It also illustrates how NPWT has transformed the management of complex wounds in veterinary medicine. A wound of this severity would previously have required lengthy hospitalisation and frequent, stressful dressing changes. Instead, Maple spent much of her recovery at home with her family, with her owners playing an active and empowered role in her care.

Histopathology had already confirmed that the original tumour was completely excised with clean margins so once the wound healed, Maple had every reason to look forward to a full and happy life.